SOME FACTS ABOUT FLYING
HAVE YOU EVER watched a balloon as it slowly meandered upward into the sky? The balloon is able to fly because the air within it…
HAVE YOU EVER watched a balloon as it slowly meandered upward into the sky? The balloon is able to fly because the air within it…
Position Summary Accommodates guests of hotel by greeting, performing guest transactions, answering the telephone, operating necessary front office equipment, etc. to ensure high-quality guest relation….
Front Office (Hotels)- Guest Relations Officer- Job Description Key Responsibilities Plan and coordinate the provision of friendly, efficient services to guests Schedule activities for guests…
The hotel industry in India thrives largely due to the growth in tourism and travel. The emergence of budget hotels in India to cater to…
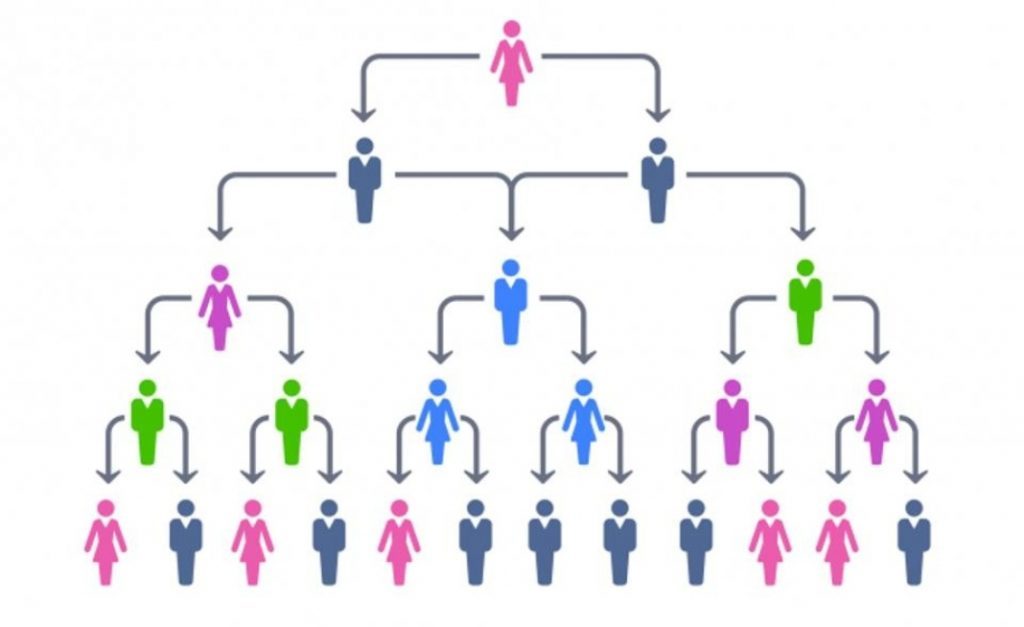
Hierarchy of Flight Crew Hierarchy varies from one airline to the other. Aircraft Crew is divided into two groups- Cockpit Crew and Cabin Crew. As an…
Cabin crew are also known as Flight Attendants, Air Hostess, Flight Stewards or even trolley dolly’s! They are primarily on board an aircraft for the…
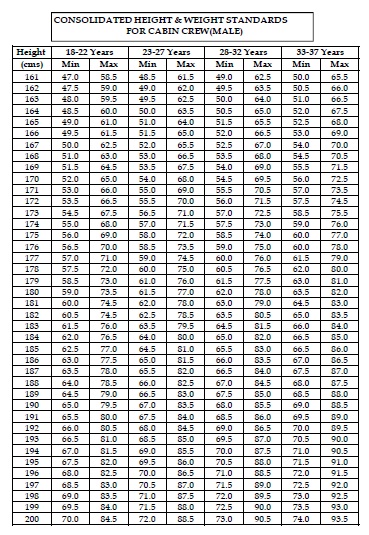
CLASS-II MEDICAL ASSESSMENT ( Applicable to Cabin Crew and Airport Ground Staff). Few of the same tests are also applicable for Hotel Staff. These requirements…
Feet/Inches -> Centimeters 4 feet 6 inches – 137 cm 4 feet 7 inches – 140 cm 4 feet 8 inches – 142 cm 4…